
Personal Information
Pain Synopsis
Back / Leg Pain
| N/A | All back pain | More back pain than leg pain | 50/50 | More leg pain than back pain | All leg pain | |
| Choose one |
|---|
Back / Leg Pain Levels (0 = no pain - 10 = constant extreme pain)
* When you have the least amount of pain, what number would that be between 0 and 10?
* When you have the most amount of pain, what number would that be between 0 and 10?
* Rate your average pain (i.e. 20 days of the month, you have a Minimum (2) pain, but 10 days of the month you have a Maximum (9) pain, therefore the Average pain may be closer to the Minimum than to the Maximum, giving you an Average of possibly (4))
| N/A | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| Minimum pain | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Maximum pain | |||||||||||
| Average pain |
Neck / Arm Pain
| N/A | All neck pain | More neck pain than arm pain | 50/50 | More arm pain than neck pain | All arm pain | |
| Choose one |
|---|
Neck / Arm Pain Levels (0 = no pain - 10 = constant extreme pain)
* When you have the least amount of pain, what number would that be between 0 and 10?
* When you have the most amount of pain, what number would that be between 0 and 10?
* Rate your average pain (i.e. 20 days of the month, you have a Minimum (2) pain, but 10 days of the month you have a Maximum (9) pain, therefore the Average pain may be closer to the Minimum than to the Maximum, giving you an Average of possibly (4))
| N/A | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| Minimum pain | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Maximum pain | |||||||||||
| Average pain |
Tolerances / Endurance ( maximum time / distance )
Personal Health Information
Case history - work involvement & leisure time activities
The physical strain in job and leisure time plays a major role for orthopedic diagnosis and therapy. This questionnaire will therefore help us to give you a proper evaluation.
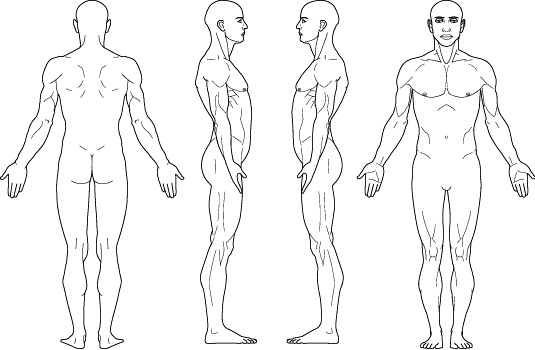
Body Scheme
1) Mark the pain area with an X.
2) Draw a line to where the pain radiates to.
3) Draw an arrow at the end of each line to show where the pain stops.
Within 5-10 business days of receiving all your data in Germany, you will receive a diagnosis and evaluation. This may be relayed through your Liaison. Therefore it is important that you stay in communication with your Liaison.
Malte Peterson -- Head of International Department -- Tel.: +49 171 3000088